3. Line of Best Fit
Epistemology, etymology, and etiology

Welcome to CHAPTER THREE of #TechnicallyAutistic: Lessons from the Periphery, where I talk about how people have diagnosed different forms of autism.
Previous chapter / Next chapter
Some of the older folks I’ve talked to will tell me aha, they know what the issue is. The issue, they say, is that I have Asperger’s and “they” have “actual autism.”
“You’re comparing yourself to people who can’t even talk, write, or go to school!,” they’d say. “Of course you’re going to feel out of place.”
It’s either that, or I have “actual autism” and “they” are diagnosing themselves because it’s trendy. “Don’t worry about what kids on TikTok are saying; they just want attention,” they’d say. “Keep listening to your parents and doctors.”
For those of you who are too young to remember, Asperger’s Syndrome was a diagnosis given to people who had more subtle signs of autism and had no language delay, before the medical community decided, never mind, that’s also autism. Anyone who was diagnosed with Asperger’s was diagnosed with autism. Kind of like how all Musical.ly users got moved to TikTok, but much more serious. Many people don’t know this, but the diagnosis got its name from Hans Asperger, who singled out a subset of autistic children who were “educable” enough to be spared from the Nazis. So not as much of a cancel culture thing if you ask me; it’s a “let’s not repeat history” thing.
Another label that is considered outdated is “high-functioning” and “low-functioning.” These labels are used as an excuse to stigmatize people and say they’re “better” or “worse.” It reminds me of how in the book Flowers for Algernon, they separated everyone in the mental institution into 'tidy' or 'untidy,’ saying that the ‘untidy’ ones were lost causes. That was a speculative novel from the 60s, and this kind of thinking has no place in 2024.
And how about someone like Elizabeth Bonker, a valedictorian at Rollins College who couldn’t talk, and gave a graduation speech through a computer? Instead, we say “high support needs” “medium support needs” and “low support needs” to focus on what they need from society, rather than how they fall short.
Oh, and also: many people on the spectrum will say that they’re “an autistic person” rather than a “person with autism” because they view autism as an crucial part of their identity, as opposed to a disease entity (Though some people still prefer “person with autism.” As you can see, I’m more used to just saying "autistic,” but will use "person with autism" if it’s called for — or if it’s the less clunky option). We also don’t use terms like “normal” or “healthy”; instead, we use “neurotypical” for those without significant neurological differences and “allistic” for those who are not autistic.
Now, as far as my little dilemma goes: I’d still have all the same questions if I replaced the word “autism” with “Asperger’s,” if I could assure people that I’m “high-functioning,” if I looked in the mirror and reminded myself that I had autism but autism didn’t have me.
If you didn’t, then now you know. While some people will see these sort of updates and see them as this scary banned words list, I see it as helpful information about our eras and the reckonings that define them.
Changing the way we speak can be a powerful act of repair, though it can also sometimes lead to the development of a euphemistic treadmill, where we get rid of hurtful words with nicer sounding ones, only for those new words to take on the same negative connotations. As cliche as it may be, you never know what anyone is going through or have gone through in life, so the best we can do is to treat people with the same respect we hope to receive.
Now, as far as my little dilemma goes: I’d still have all the same questions if I replaced the word “autism” with “Asperger’s,” if I could assure people that I’m “high-functioning,” if I looked in the mirror and reminded myself that I had autism but autism didn’t have me. I know because that was where I started.
The vastness of “the spectrum” has long fascinated the public. How can a Silicon Valley exec have the same condition as someone who cannot shower on their own and communicates through grunts? For decades, TV, news, and magazines have reduced this topic to sensationalism fodder, shrouding the real question in a veil of mystique.
We know that approximately 80 million people worldwide are diagnosed with autism. We also know that, say, Takiwātanga in Maori and 自閉症 in Japanese, both translate to autism in English. But how do we know that we’re talking about the same things?
Enter the International Classification of Diseases (ICD), an official document maintained by the World Health Organization. This document (which is available online) is seen as the constitution for the medical world and is used for insurance billing in the United States, among other purposes.
We also know that, say, Takiwātanga in Maori and 自閉症 in Japanese, both translate to autism in English. But how do we know that we’re talking about the same things?
The ICD-11 criteria for Autism Spectrum Disorder (6A02) are as follows:
Persistent deficits in initiating and sustaining social communication and reciprocal social interactions that are outside the expected range of typical functioning given the individual’s age and level of intellectual development. Specific manifestations of these deficits vary according to chronological age, verbal and intellectual ability, and disorder severity. Manifestations may include limitations in the following:
Understanding of, interest in, or inappropriate responses to the verbal or non-verbal social communications of others.
Integration of spoken language with typical complimentary non-verbal cues, such as eye contact, gestures, facial expressions and body language. These non-verbal behaviours may also be reduced in frequency or intensity.
Understanding and use of language in social contexts and ability to initiate and sustain reciprocal social conversations.
Social awareness, leading to behaviour that is not appropriately modulated according to the social context.
Ability to imagine and respond to the feelings, emotional states, and attitudes of others.
Mutual sharing of interests.
Ability to make and sustain typical peer relationships.
Persistent restricted, repetitive, and inflexible patterns of behaviour, interests, or activities that are clearly atypical or excessive for the individual’s age and sociocultural context. These may include:
Lack of adaptability to new experiences and circumstances, with associated distress, that can be evoked by trivial changes to a familiar environment or in response to unanticipated events.
Inflexible adherence to particular routines; for example, these may be geographic such as following familiar routes, or may require precise timing such as mealtimes or transport.
Excessive adherence to rules (e.g., when playing games).
Excessive and persistent ritualized patterns of behaviour (e.g., preoccupation with lining up or sorting objects in a particular way) that serve no apparent external purpose.
Repetitive and stereotyped motor movements, such as whole body movements (e.g., rocking), atypical gait (e.g., walking on tiptoes), unusual hand or finger movements and posturing. These behaviours are particularly common during early childhood.
Persistent preoccupation with one or more special interests, parts of objects, or specific types of stimuli (including media) or an unusually strong attachment to particular objects (excluding typical comforters).
Lifelong excessive and persistent hypersensitivity or hyposensitivity to sensory stimuli or unusual interest in a sensory stimulus, which may include actual or anticipated sounds, light, textures (especially clothing and food), odors and tastes, heat, cold, or pain.
The ICD also notes: “Some individuals with Autism Spectrum Disorder are able to function adequately in many contexts through exceptional effort, such that their deficits may not be apparent to others. A diagnosis of Autism Spectrum Disorder is still appropriate in such cases.”
Just like the ICD, the DSM defines autism in two core features: “persistent deficits” in social communication, and “restricted, repetitive behavior.” (American Psychiatric Association, which owns the DSM, states on its website that the DSM is “compatible” with ICD1, and lists corresponding codes for insurance billing2) DSM-5-TR is the current edition of the DSM, and it came out in 2022.
Almost everyone who fits ICD-11’s criteria for autism will fit DSM-5-TR’s criteria, except a minority of people with intellectual disabilities who may fit ICD-11’s descriptions but may not make the cut for the DSM’s criteria, which states that “social communication should be below that expected for general developmental level. Overall, the DSM uses a more standerized approach.
DSM-5-TR defines “persistent deficits” social communication (section A) by the following parameters: “social-emotional reciprocity,” which means that a person means that a person has difficulty taking turns and sharing (section A1); “nonverbal communicative behavior” which means stuff like facial expression, tone, and body language (section A2); and last but not least, “developing, maintaining, and understanding relationships” (section A3). In order to receive a diagnosis of autism, a person must experience challenges in all three areas.
When it comes to “restricted, repetitive behaviors” (section B), you only need two of four: this could be “stereotyped or repetitive motor movements” which means that a person does the same things over and over, like rocking back and forth (B1); “Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior” which means a person feels compelled to do things in a very specific way (B2); “Highly restricted, fixated interests that are abnormal in intensity or focus” which refers to having very focused interests, commonly referred to as "special interests” (B3); and/or “hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment” which means someone will seek out or avoid smells, sounds, sights, and touch that other people might not notice (B4).
Virtually everyone I know who’s been diagnosed with autism has a lot to say about the diagnostic process.
More often than not, I see the piece of paper diagnosing me as a loose thread connecting me to a bunch of discussions that often do not pertain to me. And I don’t mean to sound ungrateful because I realize that this piece of paper allows me to essential accommodation and healthcare, things people have fought for, and continue to fight for. It’s just that the diagnosis doesn’t feel very meaningful as an overarching concept. But for many others, it is meaningful.
And super personal.
At best, I have heard, it’s a long overdue confirmation of something they already know; at worst, a dehumanizing caricature of their mind. The language used in the criteria can be so othering precisely because the descriptions feel so familiar to the individual or their loved ones.
Virtually everyone I know who’s been diagnosed with autism has a lot to say about the diagnostic process.
I’ve read countless Web articles about people who struggled to come to terms with their autism diagnoses. The crux of those stories isn’t “Huh? Is this referring to me? Maybe it’s a mistake.”
Rather, it’s “This is insulting.” ‘Deficit’ according to who? ‘Failure’ by whose standards? ‘Excessive’ for what reasons?
It’s “The whole thing is a scam because if I was a little white boy, I would have been diagnosed.” But they weren’t, so I was called lazy or dramatic or hysterical.
And each one of them resolve with reclamation, aka Owning It.
(Video by @alasiabeautyy)
I don’t wait for resolutions anymore. I thought that my summer reading Pathological: The True Story of Six Misdiagnoses by Sarah Fay would give me a different perspective. The author never “came to terms” with any of her diagnoses, and that excited me. But when I came across an interview about Fay’s new book, Cured where the reporter asks if a diagnosis could ever be helpful, her response mirrored what I’d already heard before:
Definitely, and I always use the example of the autism community, because they’ve done something so important and miraculous, given our mental health system. They’ve embraced that diagnosis. They have championed each other with it, they have created the neurodiversity movement, which has said that it’s really the world’s job to not just accept but appreciate the way they see the world, hear the world, and interact with the world.
When I saw that, I couldn’t help but wonder: What’s stopping her from just saying “Hey, so it turns out I’m autistic”? If I wanted to, I could easily cherry-pick details from Pathological to suggest Fay fits the DSM criteria for autism. Just to be clear, I’m not saying that we should actually do that to people (let’s not!). I’m sure Sarah Fay is a wonderful person, diagnosis or not.
My point is that if my only qualm with the diagnosis was that it was “too pathologizing”, I wouldn’t be having this conversation. There are plenty of other reasons that might make a person decide that a label isn’t right for them, or sit on the fence.
It’s just that the diagnosis doesn’t feel very meaningful as an overarching concept.
I was born at the cusp of the “different, not less” generation. My TikTok keeps showing me “neurospicy” content. Most of my therapists put air quotes on subjective words like “excessive” and replace the words failure and deficit with differences and needs when we review medical literature. And guess what? I still have questions.
When I first started brainstorming this project over a year ago, I conceptualized the competing definitions of autism into a Venn diagram, where one circle represented “people who act autistic,” meaning individuals who exhibit the behaviors described by the DSM or the ICD, and the other, slightly larger circle represented “people who think autistic” meaning individuals who identify with the underlying internal processes shared by a good majority of the first group.
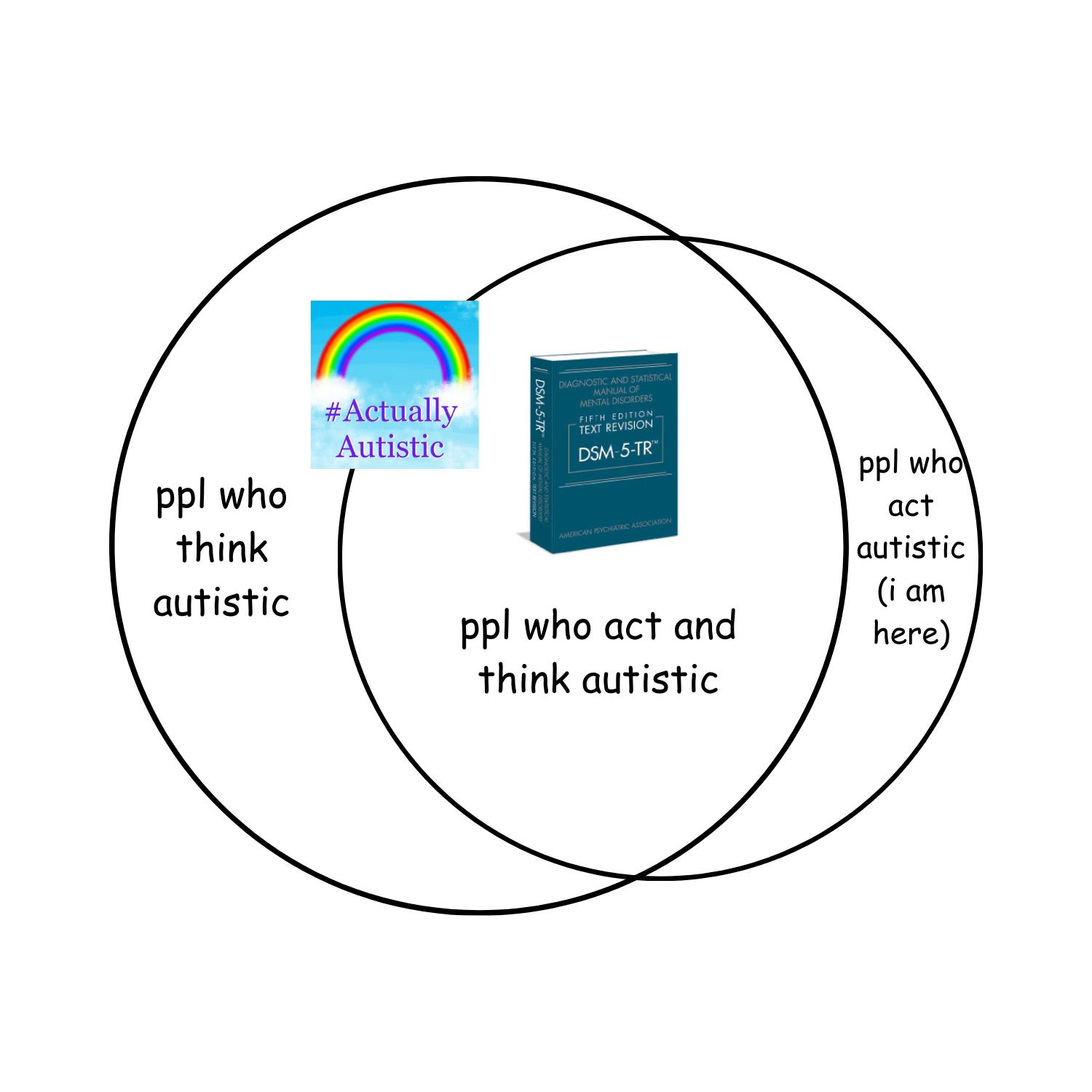
The reality, of course, is much more complicated.
DSM-5-TR states that a person may exhibit symptoms of autism “currently, or by history.” In other words, both observations from the past and the present may be counted towards this diagnosis. Based on this alone, I assumed that the DSM’s definition of autism had everything to do with how you act, and nothing to do with how you think. After all, many people have life milestones delayed by other factors and undergo seasons of life catching up, building armors, and questioning other people’s expectations; if the DSM allows you to cherry-pick potentially unrelated behaviors and call them autism, that tells me that autism is a quantitative phenomenon and not a qualitative one.
Comimg from someone who’s not neccesarily learning about this from a scientific and medical standpoint, I don’t know how people can even begin to pinpoint autism.
Upon a closer examination, I found statements in the criteria that suggest otherwise. For example, it says that “Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities or may be masked by learned strategies in later life).” Again, it’s saying that if you exhibit symptoms of autism at one point, you can still get a diagnosis even if those symptoms later disappear. But it’s also saying that there has to be a reason. So which capacities are considered to be “limited,” and what exactly is being masked?
Comimg from someone who’s not neccesarily learning about this from a scientific and medical standpoint, I don’t know how people can even begin to pinpoint autism. I mean, the variables are pretty wild. Every autistic operson I’ve spoken to has “other stuff” going on—studies show that at least 70% of autistic people have at least 1 other mental disorder3. And according to the CDC, 37.9% of children diagnosed with autism also meet the criteria for an intellectual disability4.
I do know, however, that when doctors evaluate school-aged children for autism, they’ll usually administer an IQ test along with some math, reading, and writing problems, even though none of those tests directly assess the symptoms outlined in the diagnostic criterias. This gives them a better idea of how the child operates, compared to other kids who are similar to them. These diagnoses can be arbitrary because they’re based on social constructs and may involve flawed methodology, but that’s not the same as it being random. It’s not something that is given with zero thought.
Some people may not realize this, but much of what we’ve come to understand as progressive views on autism were spearheaded by individuals who had already been formally diagnosed. This includes Temple Grandin, diagnosed at age 3 in 19505, Donna Williams, diagnosed in her 30s in the 19916, and Kassiane Sibley, diagnosed at age 3 in 1985 (and later determined to be an “autistic savant”).7
All of these voices had the remarkable ability to fill the vacuum. Though Grandin has been guilty of spreading some very harmful ideas8, her advocacy was considered groundbreaking in the 90s; when her book, Thinking in Pictures, came out in 1995, that was the first time people saw a firsthand account of how the autistic mind does work, as opposed to how it doesn’t work. She explained, for example, that it takes her longer to decipher what people are saying, or learn how to use words correctly, because she thinks in such a visual way.
Unlike those of most people, my thoughts move from video like, specific images to generalization and concepts. For example, my concept of dogs is inextricably linked to every dog I've ever known. It's as if I have a card catalog of dogs I have seen, complete with pictures, which continually grows as I add more examples to my video library. If I think about Great Danes, the first memory that pops into my head is Dansk, the Great Dane owned by the headmaster at my high school. The next Great Dane I visualize is Helga, who was Dansk's replacement. The next is my aunt's dog in Arizona, and my final image comes from an advertisement for Fitwell seat covers that featured that kind of dog.
With her writing, Grandin pioneered the market for autism memoirs, inspiring generations of people to open up and share their journeys. Today, a record number of adults are seeking diagnoses for themselves.





(Graphic by The Neurocuriosity Club/@theneurocuriosityclub)
But who knew that there might not actually be an “official checklist” for autism? The ICD says that autism “may include” the behaviors they list out, and even the DSM notes that their examples are “illustrative, not exhaustive.” Both texts use the word “manifest.”
According to the Oxford Learner’s Dictionary, manifestation is “to show something clearly, especially a feeling, an attitude or a quality.”9 So basically: when every time the ICD or the DSM mentions a symptom of autism, it’s up to us (particularly, the people who do the diagnosing) to add “—or something along those lines.”
So basically: when every time the ICD or the DSM mentions a symptom of autism, it’s up to us (particularly, the people who do the diagnosing) to add “—or something along those lines.”
Of course, that begs the question: Where are those lines pointing to?
Thank you for reading CHAPTER THREE of #TechnicallyAutistic: Lessons from the Periphery. Just a friendly reminder that this blog series is a work of MEMOIR. All pertinent disclaimers apply, such as:
- My narratives reflect the cultural context of the present year (2024? No way!) and my experience of growing up in the 2010s. If the world doesn’t change and I don’t change, then I’d be damned—we’d all be. Stay curious.
- I’ve made minimal changes to some names* and identifying details for the sake of privacy. I’d rather you not stay curious about that.
- I also used fictional names* for medications because different things work for different folks and I don’t want to interfere with anyone else’s path to wellness. (Do I have to tell you that I’m not a doctor?)
- But yes, this series contains depictions of mental illness that some readers may find triggering. Please take care of yourselves.
Now that I got that out of the way, a special shout-out to the best accountability buddies in the world: Dr. Harriet Hustis, for allowing me to start this project in a life-changing summer program, Nora Neus/The Longform Lab for supporting me through completion, and the journalism faculty of TCNJ for setting me up for success.
Next chapter:
Previous chapter:
https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM_Insurance-Implications-of-DSM-5.pdf
https://www.psychiatry.org/psychiatrists/practice/dsm/updates-to-dsm/coding-updates/2021-coding-updates
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6669096/#:~:text=Previously%20reported%20prevalence%20rates%20indicate,of%20children%20and%20adolescents%20with
https://www.cdc.gov/autism/communication-resources/addm-network-factsheet.html#:~:text=Among%208%2Dyear%2Dold%20children,with%20children%20born%20in%202012.
https://med.stanford.edu/news/all-news/2014/11/5-questions--temple-grandin-discusses-autism--animal-communicati.html#:~:text=Born%20in%201947%2C%20she%20was,University%20of%20Illinois%20in%201989.
https://en.m.wikipedia.org/wiki/Donna_Williams#:~:text=In%201991%2C%20Williams%20was%20diagnosed,t%20have%20known%20about%20...
https://www.forbes.com/sites/alicegwalton/2011/12/09/living-life-with-autism-ii-perspectives/
https://intheloopaboutneurodiversity.wordpress.com/2019/07/21/why-temple-grandin-is-not-my-hero/
https://www.oxfordlearnersdictionaries.com/us/definition/english/manifest_1